
My Spinal Fusion Experience
In May 2021 I had a lumbar inter-body fusion at 30 years old to address a 15-year recurring disc herniation between my L5/S1 vertebrae.
Going into the surgery I found information about the procedure was either too technical or academic to easily understand, too sales-oriented for a particular device or procedure or hospital, or in video-anecdote-form on YouTube, so I felt compelled to write about my personal experience.
Below is some background, a description of the procedure I had, my experience recovering after surgery, as well as some tips I picked up and mistakes I made with the hopes of making it easier to manage for others considering a similar procedure. In a few months I’ll add more to the story after (hopefully) recovering more completely.
None of this is medical advice, most is just therapeutic journaling.
TL;DR
If you get bored and don’t finish the whole post, take away the following highlights/recommendations:
- I had a recurring disc herniation due to degeneration, which was doomed to disrupt my life regularly for years until it naturally fused. Surgical fusion was agreed upon by all three doctors I consulted.
- I could walk a tiny bit the day after surgery. Within a week I could walk for 30m before I had too much pain. Within two weeks I could walk for an hour and felt stronger every day.
- I could not do basic housework, prepare food, or even manage pain for the first week without my wife helping me with literally everything, even getting in and out of bed.
- I used a walker extensively for the first week, and a claw-style grabber for the first two weeks.
- I messed around with bed pillows a ton until I found a position where my legs and back were comfortable. I wish I had just bought a wedge pillow.
- A toilet seat riser and safety rails were very helpful as I couldn’t bend with my torso at all for some time.
- I could not twist, bend, or lift anything more 5 pounds for two weeks, and had a lot of trouble reaching up. I couldn’t bend enough to spit toothpaste when brushing for a week.
- The “Log roll method” of getting in/out of bed was really important. When I forgot or was lazy and twisted even a little it hurt like hell. For the first four days, my wife had to lift my legs because I couldn’t pull them up onto the bed myself.
- I rapidly recovered in the first twenty days from 1/10 to 6.5/10.
- Two years later, I’ve recovered about 90% of my typical body/athletic ability. See the last section for a brief update.
Nerve pain history
I describe my pain as persistent stabbing, tingling, shooting, and throbbing that would radiate from my low back just above my belt, down through my thigh and into the lateral left calf muscle. My left calf muscle would twitch, spasm, flutter, and was overall very distracting all the time.
At its worst, I developed a limp and foot drop due to near-zero strength in my left calf and ankle. My left foot would feel cold itself but warm to my hands (very weird) and its touch sensation was muffled or muted as if I was wearing five pairs of socks at the same time. Sitting or standing for long periods would exacerbate symptoms enough to bring tears. I would frequently wake up yelling about some monster in my dreams that was gnawing on my left leg, only to find my calf had turned into a knotted baseball-sized mess.
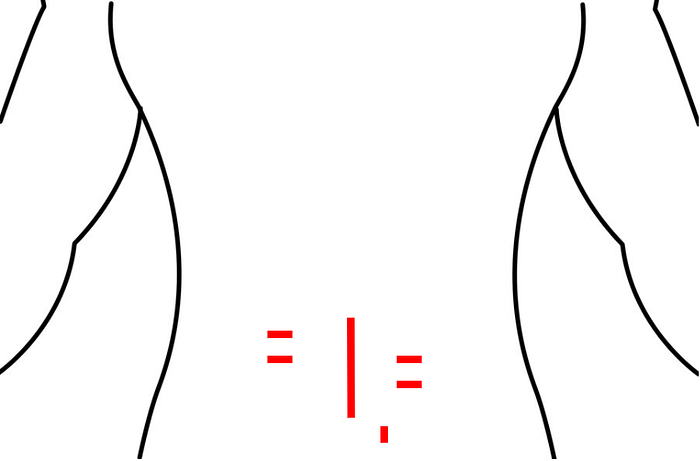
The pain almost perfectly followed the red/yellow L5 and S1 dermatomes below:

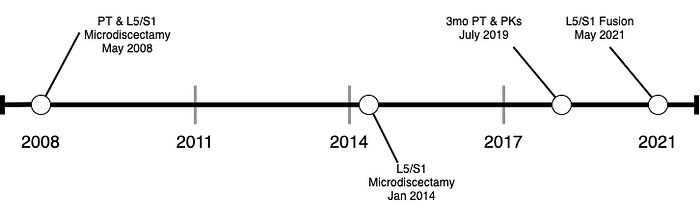
I first developed symptoms in 2008 at age 15 with no obvious cause, though I can recall falling from a height of 15–20 feet and getting in a violent pick-up football tackle the year or two before. Every few years since, I cycled through periods of relatively no pain to major flare-ups requiring strong pain killers, physical therapy or surgery. Each noted date below was accompanied by months of being mostly dysfunctional, missing class, work, and sleep.
Symptoms prompting fusion in 2021
In 2021 my nerve pain symptoms deteriorated to the worst and most painful they have ever been, by far.
I was down in bed in mid-March on my back with ice packs and painkillers. From March 20th through May I was in bed almost all day every day, leaving bed only for doctor’s appointments and bio-necessaries. Standing for more than a few minutes was excruciating and would bring me to tears.
In the below graph, my steps activity graph (blue) shows this pretty clearly — I went on my 5-mile run and 3–4 mile walks the next few days (which is a typical day for me), then my activity fell off a cliff. Once I realized I had herniated my disc again I started logging my pain (pink) on a 1–10 scale. Through all of April, I rarely breached 1,000 steps, which is essentially walking around the house a few times in a day.
I went to a sports medicine doctor at the University of Washington I had dealt with before and was prescribed an MRI looking for a herniated L5/S1 as I had in years before. I was told by the doctor and his colleague that I had the biggest herniation they had ever seen (yay), and it’s pretty obvious from the image. I was referred to a surgeon for urgent surgery.


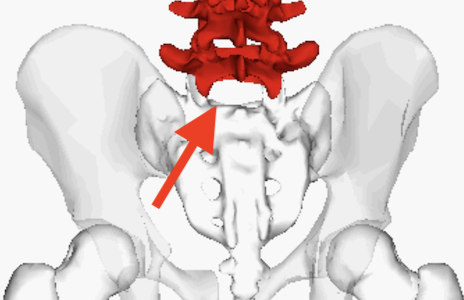
For reference, the L5/S1 is the white area between the lowest lumbar vertebrae and the sacrum near the hips:
I visited two surgeons over the next two weeks, both of which agreed on fusion.
Decision for fusion over other options
When I was trying to figure out what to do to relieve my back pain, I had a few options:
Option 1: Physical Therapy Only
This option would just be to go to PT for a few months and manage pain with strong pain killers. This was attractive because I’d recovered from a herniated disc from surgery twice already, but also once before just by using a few months of PT and PKs. I chose not to do this for a few reasons. First, my pain was bad enough that I felt like I needed relief sooner than I was willing to wait with PT, so I was biased for a surgical option. Second, I was hurting so bad that I could not sit, stand, or walk long enough to even get to a PT’s office.
Option 2: A Third Microdiscectamy
This option would be to have a third microdiscectamy, yet again shaving the herniated part of my disc away that was causing me pain. This was attractive because I’d had the procedure twice before already and understood the out-patient recovery and the pros/cons.
The primary reason I didn’t choose another microdiscectamy was because of a study my surgeon cited that linked the size of ligament tear with risk of re-herniation.
In my case, I now had a “…left subarticular disc extrusion … measuring 14 mm in size..” which is a very large tear. Combined with the fact that I’d already had two microdiscectamies in the past and “..this will probably be [my] sixth disk herniation..”, and yet was still in this situation a few years later, my surgeon and a second opinion agreed that I was extremely likely to repeatedly have re-herniation again and again and again until there wasn’t any disc left, so why bother?
Option 3: Total Disc Replacement (Artificial Disc)
This option would be to have an artificial disc inserted between my L5 and S1 vertebrae, much like an artificial hip. This was attractive because artificial discs allow for a much wider range of motion than other invasive options like fusion.
I opted against this option for a few reasons as well. First, according to my surgeon, this option doesn’t have a major advantage in success rate or patient-reported quality of life compared to standard inter-body fusion, but is carries risks of mechanical failure over time. Second, at the level that I needed correction, L5/S1, there isn’t a lot of movement anyway, so the cost/benefit wasn’t there. If I was dealing with a disc in my upper back or neck, then it would have been a different story.

Option 4: AxiaLiF
AxiaLiF is a form of inter-body fusion that is the least-invasive. Colloquially called “the butt screw,” a big titanium screw would be driven upwards from the tailbone area, fusing the vertebrae together. My surgeon recommended against this as it was associated with increased infection rates over a standard fusion, and was no longer even practiced locally after so many occurrences of complications.
Option 5: Lumbar Interbody Fusion (selected)
This was the option ended up going for, described later in the Procedure section.
Doctor’s Opinion
I got three opinions that all agreed that fusion would be a good way for more long-lasting relief of my nerve pain symptoms. If you’re considering fusion, I’d definitely recommend getting a second opinion because while each doctor agreed, they all had different things to say about it.
Personal Anecdotes on Recovery from YouTube
Leading up to surgery, I viewed dozens of YouTube videos of personal testimonials covering the recovery process to prepare myself for what I should expect. A few of my favorites were Derek Spratt’s, Will Port’s, and Emily Baker’s, as they followed up with their recovery and challenges periodically over several years post-op, which gave me confidence that I could return to a normal life after surgery.
These were all very helpful and contained a lot of the same tips I mention elsewhere, I’d recommend anyone considering fusion to check these out.
Risks of Fusion
The risks with that I could gather were infection, no change in pain, worse pain, paralysis, and death.
Failed Back Syndrome — Unchanged or Worse Back Pain
A worrying risk was Failed Back Syndrome, also called “post-laminectomy syndrome.” This risk is essentially that something goes wrong during surgery, or that the surgery doesn’t actually fix the underlying issue. Usually this is caused by a surgeon’s mistake, scar tissue forming in a way that re-aggravates the nerves, a missed portion of the herniation that ends up floating around, blocking the bones from fusing, or poor healing due to other health issues.
Death
Obviously, the worst risk was death. One study I found showed a 0.18% death rate of fusion in the males included in the study. This is just a little less than one in five hundred — which was really worrying! After further reading and discussion with my surgeon, though, I felt better about the risk. The study I read first included people of all age ranges, and varying degrees of health. The median age for the surgery I was having is much higher than my own, and the risk of complications is higher as you age. At my young age and good general health, I would be most likely to die from overdosing on the opioid pain killers prescribed after surgery than any other complication.
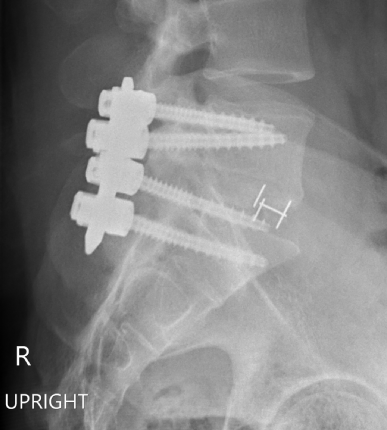
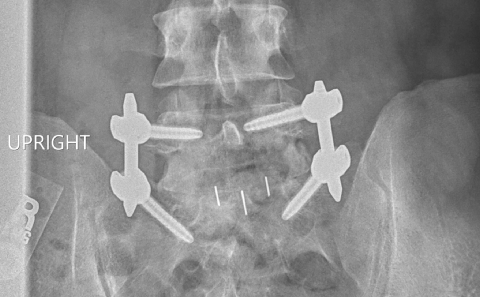
Procedure — TLIF
The procedure I had was a Transforaminal Lumbar Inter-body Fusion (TLIF). I was in the operating room for four hours. I have six incisions — one vertical six-inch incision that re-used and extended a scar from a previous microdiscectamy, four straddling horizontal two-inch incisions, and another small vertical incision on the bottom right. Oddly enough the four horizontal incisions don’t line up vertically with each-other (I’m not sure why).
The four two-inch horizontal incisions were each used to insert a total of four 50mm titanium screws tying the L5/S1 together, acting as a cast to keep everything from moving while the bones fuse together.
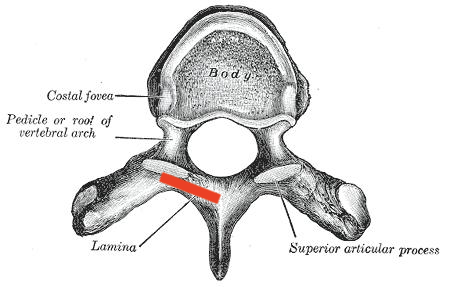
The large vertical incision was used to perform a laminectomy, which is where the bone that connects to the poke-y ridge you feel when you touch your back to your vertebrae is removed to decompress the nerve (red line below).
The facet joint, which is the joint between the levels of above-mentioned “bony projections” was also removed, the “extremely large extruded [disc] fragment” pinching my nerve was removed, followed by the removal of what was remaining of my L5/S1 disc.
Then a crescent-shaped polyetheretherketone plastic spacer was placed between the two vertebrae along with Infuse bone-growth material to help the bones grow together.

After the spacer was in place, two 40mm rods were placed through the left and right side incisions and torqued into place.
The below X-ray shows the screws, rods, and spacer. The small wire “H” is an X-ray-visible marker within the plastic spacer.
Recovery
I recovered back to a sustainable quality of life way faster than I thought I would, really turning the corner at the two week mark. The first three days was a total blur and an all-around awful experience, but I was able to do more and more every day following that.
Immediately upon waking up from anesthesia I tested if my legs still worked. I was really worried about becoming paralyzed during surgery, but was relieved that they felt fine. I think I told my nurse this about a thousand times as I was coming to.
Then I took note of my left leg that had been causing me pain recently:
I felt, for the first time in years, absolutely no nerve pain in my leg. It was incredible. The touch sensation in my left foot was much stronger, though not perfect, and it no longer felt cold and distant. The sharp tingling pins and needles in my ankle was gone, and my left calf had stopped spasming.
I get chills every time I think about that first realization.
I did feel intense pain elsewhere, though, the worst I’ve felt in my life even with IV pain killers and local anesthesia.
My calves were painful due to electromyographic needles inserted into my legs to measure the health of my nerves during the procedure. This faded somewhat after a few days but still bothered me even two weeks later, and was weirdly the last thing to recover fully.
It felt like a horse kicked me in the chest from being laid on my front in a harness for so long, but this went away by the next day.
My lateral left thigh was almost completely numb, to the point of barely sensing someone touching it, but also painful. My surgeon said this was normal as the nerves are stretched by the new spine height that the spacer provides. This mostly recovered within a week, though is still somewhat noticeable two weeks later.
I also had absolutely zero strength in my torso and a lot of pain around the incisions, glutes, and hips. I didn’t get out of bed at all the first day. If I wanted to adjust or roll even slightly while in bed, I needed to use my hands under my hips to “walk” my torso into position. Moving enough use a urinal was extremely painful and difficult.
Week One At Home
The first day back at home, the day after surgery, I slept almost all day and just laid in bed taking pain killers every few hours. Days two and three were about the same.
After four days I could get out of bed by myself with a walker to use the restroom. Before that my wife needed to help me get out of bed. I had to move really slowly and with a walker — it took me about ten minutes just to get out of and back into bed.
After five days I could stand up long enough to eat meals.
After six days I was just able to walk very gingerly around one city block with help.
After eight days I was able to go for a half-hour very slow and very flat ten-block walk by myself with a cane. I also was able to sit for ten minutes until it was too uncomfortable.
The below graph shows my average daily pain (pink), mood (green) and activity (blue) in the first week after my surgery (May 26th). My pre-op pain level of 1 spiked to 8, then ramped down through the next few days.
As for sleep — I barely slept the two nights after surgery, showed below, but paid back the debt the following day with a whopping 17 hours of sleep. For the rest of the week, I slept from 11–14 hours per night (I average about 7.5 usually), then snoozed a little during the day.
Below shows my sleep as recorded by Autosleep on iOS (right, green), vs pain (left, pink):
Gut Health
I won’t go into a lot of detail, but as is common in surgeries involving anesthesia, my gastrointestinal system was… let’s say sleeping… until day four. Hurray for Miralax and fiber!
Getting In and Out of Bed — “Tea Pot” Method
The hardest thing to do the first few days was get in and out of bed. An occupational therapist that visited me after my surgery taught me the “Log Roll Method,” to ensure my spine stayed straight during the crucial first few days of healing.
To get into bed, you start by lowering yourself to a sitting position. Then you put your arms up toward the pillow, swing your feet up, bringing you to a side laying position. Then you roll your shoulders, hips, and knees all at the same time onto your back to avoid twisting your back.
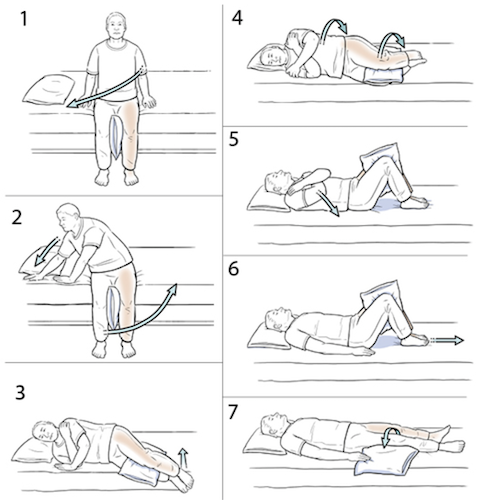
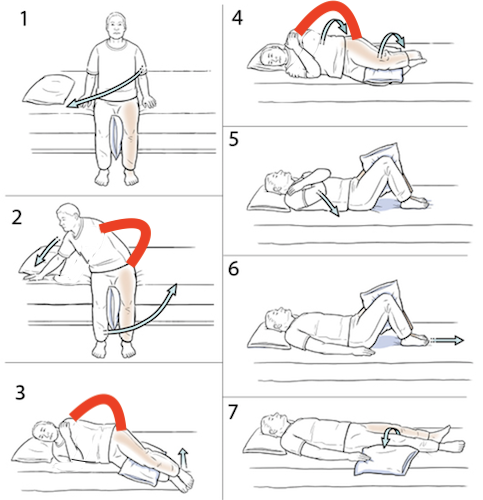
I found that instead of using both arms against the bed surface to support my body, as I was directed and shown above, it was much better to place what would eventually be the “top” arm on my hip (left arm in the diagram), using it to lock my hips and shoulders in the same rotational plane, like a car differential. It makes you look like you’re doing the “this is my handle” part of the “I’m a little teapot” kids dance too as a bonus. I found that this was way less painful getting into bed because I could use the strength of my arm and shoulder to keep my back from twisting instead of my useless low back, abdominal and hip muscles.
Please forgive the photoshop horror, but below is what I mean —the red line is the “tea pot handle” arm that locks your shoulder and hip planes together, preventing a twist:
Pain management
I found that taking pain medication on a tight schedule was really important, especially through the night. It’s way better to wake up three times at night to an alarm to take meds for one minute than to wake up in agony because there’s no painkillers in your system. It was also important to write down what I was taking when, as I was in a haze and not able to remember.
By the time I got home, I was on:
- 5mg oxycodone, 4hr interval
- 50mg tramadol, 4hr interval
- 300mg gabapentin, daily
- 1000mg tylenol, 8hr interval
- 15mg cyclobenzoprine, daily
and I progressively took less and less of the opiates over time.
I also noticed that pain had a delayed onset. I would be in bed feeling a 4/10 pain and get up to go shower. In the shower I would feel 5/10, and get back in bed at a 5/10. Then the pain would continue to get worse for up to an hour afterwards up to a 7/10. This made it tricky to know when to stop doing something — if I wanted to avoid feeling more than 6/10 pain, I really have to stop when I feel 4/10 pain, and let my body catch up.
Resting in Bed — Get a wedge pillow!
For the first few weeks I spent almost all day and night in bed, so getting it set up and comfortable really improved my quality of life.
Getting my legs adjusted so my knees were up just above chest-height to relieve pressure on the low back was really helpful. The bed at the hospital was adjustable so I could get it just right with a remote. Back at home, though, I needed to set up some pillows to get my legs supported to get the pressure relief I needed.
I started with one pillow, added a folded comforter underneath later, then two pillows and blankets eventually landing on a whole big mess to get the shape that helped. I used a rolled-up towel on each side to keep me from rolling while sleeping, as any twisting felt horrible. After a ton of experimentation, I ended up with this:

…which is basically the same shape as cheap post-surgery pillows available on Amazon. Looking back I really wish I had bought something like this:

One annoyance I dealt with in the first week was not being able to lay on my side (per surgeon’s recommendation), which is how I normally sleep. After a day or two of being on my back all day I was pretty uncomfortable.
Week Two At Home
I drastically “turned the corner” two weeks after surgery, reaching the point of feeling generally better than I did before surgery at the two-week mark, though still unable to sit comfortably for more than a few minutes.
I could start to use a laptop in bed for more than a few minutes without it being too uncomfortable.
By the two week mark I was hitting consistent 1/10 or 2/10 pain with painkillers. I did an experiment one day to see how I felt without taking any painkillers at all, but was pretty uncomfortable by the end of the day so I went with just halving everything instead (you can see the mood dip in the below graph).
I saw my surgeon for a follow-up two weeks after surgery and they were happy with how I was recovering. I got prescribed with 8 weeks of PT twice a week and was told I could start sitting up for longer and I could (finally) lay on my side.
The below graph shows my decrease of pain and then rapid increase in activity through the second week.
Conclusion, 20 Days After Surgery
As of this writing, 20 days after surgery, I can say that I feel much, much better than I did going into all this, and if I had to do it again I absolutely would.
The first week was a major bummer. However, getting better every day and being able to walk enough to consider it decent exercise I feel much stronger and more human again.
I can now sit comfortably for 1–2 hours, which is already an improvement over pre-surgery. I still can’t bend much (nor should I), so I still need help with a few things around the house that I would normally do (like reaching in the back of a low cabinet, emptying the bottom shelf of the dishwasher, etc).
It’ll be interesting to see how long until I feel comfortable working out, lifting and carrying.
Conclusion, 2.5 years After Surgery
As of today, a little more than 2.6 years later (Fall 2023), the surgery was, I’d say, a massive success. I’m back at ~90% of my typical athletic/body ability, and don’t really think about my back much day-to-day.
I am not as flexible in either twisting or bending as I once was, but I’m happy with the tradeoff of little to no pain when sitting, standing, or sleeping. For example, I used to be able to touch the floor under my toes without much issue, but now I can get about down to my ankles. I used to be able to do a total back bend, but now wouldn’t even try it.
I will occasionally have slight flare-ups, where I feel uncomfortable down my leg/calf again, particularly if I lift unsafely, work hard, or sit for many hours in a day for a few days. For example, splitting firewood is fine, but bending down weeding can cause a flare.
But the current flare-ups, which last a day or so, are 1/10 of the pain I used to feel all day, all night, every day, so it’s mostly just mild occasional, much better, annoyance. Sitting on long plane flights is still pretty uncomfortable, but not quite the absolute hell it once was.
I don’t think I’ve had any knock-on effects, such as poor posture, change in gait, etc — my body has adjusted well to the slightly less flexibility.
